
مقدمة
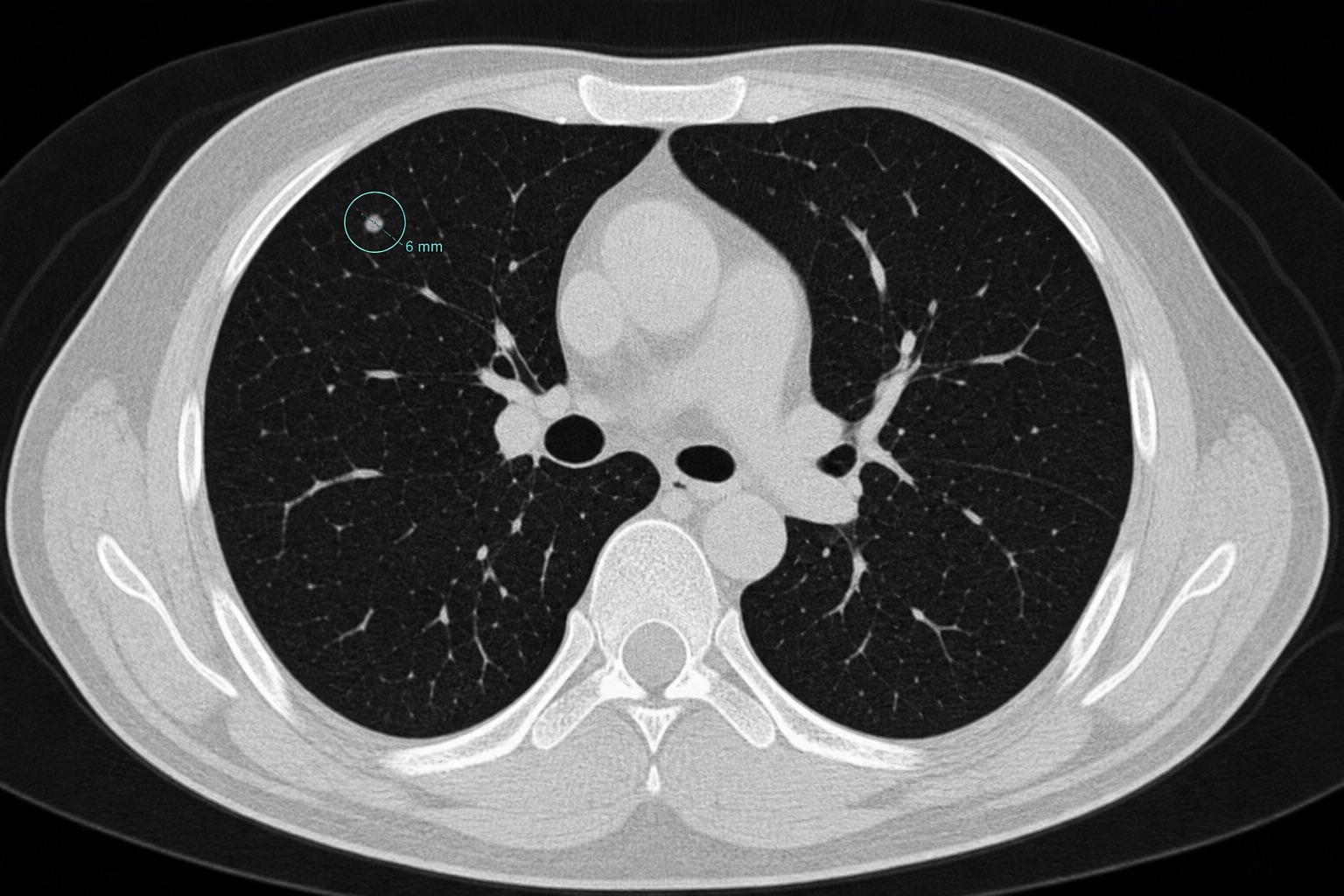
العقيدة الرئوية هي بقعة مستديرة أو بيضاوية على الرئة يبلغ قطرها 30 ملم أو أقل. معظم العقيدات حميدة، وتمثل ندوبًا قديمة أو عقدًا ليمفاوية أو التهابات.
دليل متابعة حجم العقيدة (معايير فليشنر)
- أقل من 4 ملم: خطر منخفض للورم الخبيث (أقل من 1%). لا تتطلب المتابعة الروتينية بشكل عام في الأفراد ذوي المخاطر المنخفضة.
- 4 إلى 6 ملم: إعادة فحص بالأشعة المقطعية بعد 12 شهرًا للتحقق من الاستقرار.
- 6 إلى 8 ملم: إعادة فحص بالأشعة المقطعية بعد 6-12 شهرًا، ومرة أخرى بعد 18-24 شهرًا.
- أكبر من 8 ملم: زيادة الخطر. يتطلب متابعة أدق بعد 3 أشهر، أو فحص PET-CT، أو خزعة نسيجية.
Frequently asked questions
مقالات ذات صلة
كيفية قراءة التصوير المقطعي المحوسب: دليل المبتدئين
تعلم كيفية قراءة التصوير المقطعي المحوسب خطوة بخطوة: الشرائح المحورية، والمناظر الإكليلية والساجيتالية، ووحدات هاونسفيلد، وإعدادات نافذة التصوير المقطعي المحوسب، والتشريح الرئيسي، والعلامات الحمراء العاجلة.
كيفية قراءة التصوير بالرنين المغناطيسي
تعلم كيفية قراءة التصوير بالرنين المغناطيسي بلغة مبسطة: T1 مقابل T2، FLAIR، DWI/ADC، تعزيز التباين، مستويات الصورة، القطع الأثرية، ومصطلحات التقرير.
كيفية قراءة الأشعة السينية للصدر
تعلم كيفية قراءة الأشعة السينية للصدر باستخدام طريقة ABCDE المنهجية: جودة الصورة، مجرى الهواء، الرئتين، حجم القلب، الحجاب الحاجز، التشوهات الشائعة، والعلامات الحمراء.