
허리 디스크 탈출증이란 무엇인가요?
척추 뼈 사이에는 완충 작용을 하는 디스크(추간판)가 있습니다. 이는 안쪽의 말랑말랑한 수핵과 바깥쪽을 둘러싼 단단한 섬유륜으로 구성됩니다. 섬유륜이 찢어져 수핵이 삐져나오며 척추를 지나가는 신경을 누를 때 통증과 엉치에서 다리로 뻗치는 방사통(좌골신경통)이 유발됩니다. MRI는 디스크 돌출 부위와 신경 압박을 평가하는 최선의 정밀 검사입니다.
MRI 상의 디스크 탈변 양상 단계
요추 MRI의 측면(시상면) 및 가로(축상면) 단면을 통해 디스크의 퇴행 진행 단계를 다음과 같이 분류합니다:
- 디스크 팽윤 (Bulging): 섬유륜이 찢어지지는 않고 전체적으로 둥글게 밀려나온 상태. 노화에 의한 초기 변화이며 대개 신경 압박이 심하지 않습니다.
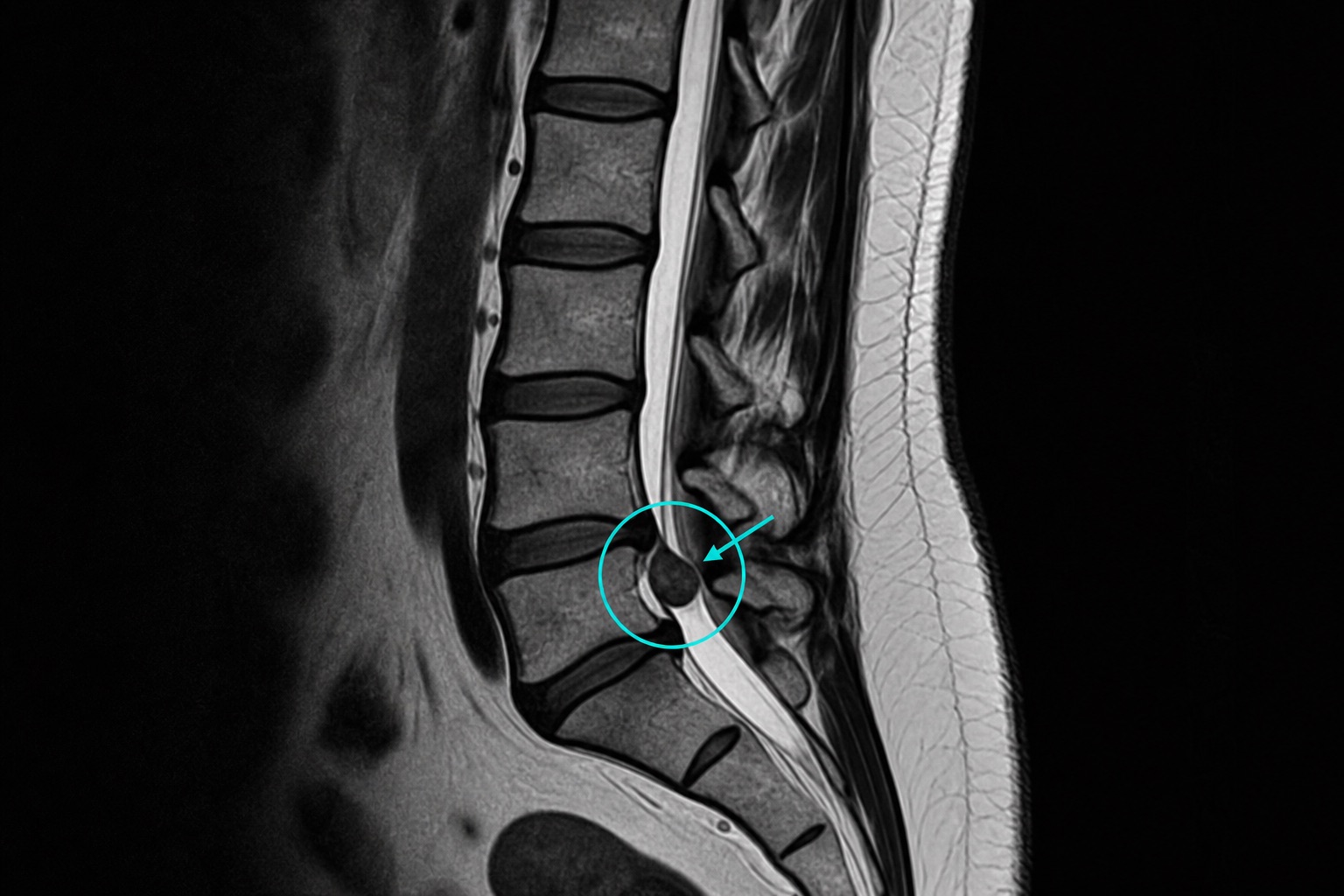
- 디스크 돌출 (Protrusion): 섬유륜의 국소 틈으로 수핵이 튀어나와 뭉툭하게 신경을 건드리기 시작한 단계. 다리 저림을 유발할 수 있습니다.
- 디스크 탈출 (Extrusion): 섬유륜을 뚫고 삐져나온 수핵 조각의 폭이 넓어져 신경을 심하게 짓누르는 단계이며, 일부는 디스크 몸체와 끊어져 척추관 내부를 흘러 다니기도 합니다(유리형 탈출).
Frequently asked questions
관련 기사 추천
CT 스캔 읽는 방법: 초보자 가이드
CT 영상의 단계를 알아봅니다: 축상면(Axial), 관상면(Coronal), 시상면(Sagittal) 슬라이스, 하운스필드 단위(HU), CT 윈도우 설정, 핵심 해부학 및 응급 징후。
MRI 스캔 영상 읽는 방법
MRI의 시퀀스를 쉬운 언어로 이해해 보세요: T1 vs T2 강조영상, FLAIR, DWI/ADC, 조영제 증강, 영상 단면, 인공물 및 보고서 용어。
흉부 X-ray(엑스레이) 판독하는 방법
ABCDE 계통적 방법을 사용하여 흉부 엑스레이 읽는 법을 배웁니다: 화질, 기도, 엑스레이 촬영 부위, 심장 크기, 횡격막, 흔한 이상 소견 및 주의 징후。